
Learn about the clinical forms of ARDS
Adult acute respiratory distress syndrome (ARDS) is a clinical syndrome with rapid onset of severe dyspnea, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
1. Causes of ARDS
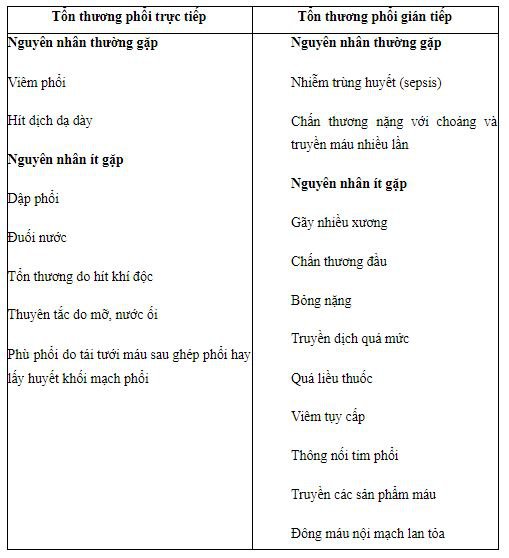
ARDS due to diffuse lung injury is caused by many underlying medical and surgical conditions. Of the many diseases associated with the development of ARDS, more than 80% of cases are due to: severe sepsis, bacterial pneumonia (40-50%); injury; too much infusion; aspiration of gastric juice and drug overdose.
Among surgical causes, pulmonary contusion, multiple fractures, and chest trauma are common causes; while head trauma, drowning, inhalation of poisons and burns are rare causes. The risk of developing ARDS is increased in patients with more than one risk factor.
Several other factors are associated with the development of ARDS such as older age, alcoholism, acidosis and severity of the disease. Trauma patients with an APACHE II score ≥ 16 have a 2.5-fold increased risk of developing ARDS, and patients with a score > 20 have a threefold greater rate of ARDS than patients with an APACHE II score < 9.
2. Clinical forms of ARDS according to disease progression stage
Clinically, the progression of ARDS also occurs in 3 phases: onset, full development, and recovery.
2.1 The onset phase The onset phase corresponds to the acute inflammatory and exudative phase of ARDS. Acute inflammatory and exudative lesions occur almost immediately following the impact of the pulmonary injurious agent and progress over a period of one week. However, studies have shown that most clinical manifestations of ARDS usually appear within 3 days after the impact of the lung injury factor.
According to the Stapleton et al. cohort study, of the patients who progressed to ARDS, 76% progressed to ARDS before 24 hours and 93% of patients progressed to ARDS before 72 hours. Time to onset in the group of patients with direct lung injury.
(0 - 2 days) seems to be lower in the indirect lung injury group (1 - 5 days). During the onset, besides the clinical symptoms of the disease that is the cause of ARDS, the symptoms The onset of ARDS is often nonspecific. Onset is marked by the appearance of new respiratory symptoms such as dyspnea, tachypnea, inspiratory muscle contractions, and auscultation of the lungs that may have moist rales along with diffuse lesions on radiographs. For patients with pre-existing respiratory or congenital heart disease, who are being treated with oxygen or mechanical ventilation, the diagnosis of ARDS should also be considered if the respiratory failure is rapidly worsening and lesions are present. new, diffuse bilateral chest radiographs and rapidly progressing.
2.2 Full-blown stage The full-blown phase corresponds to the proliferative lesion stage of ARDS. This phase usually lasts for 1 to 2 weeks depending on the patient. By the time they enter the full-blown stage, most ARDS patients require oxygen support or artificial ventilation because of severe hypoxia.
The patient's concept of "inert hypoxemia" in this period refers to the difficulty in improving the patient's blood oxygen. Conventional measures in mechanical ventilation such as increasing inspiratory pressure, increasing PEEP, even increasing FiO2 do not improve the patient's oxygenation status.
Clinically noticeable signs include: the patient is more cyanotic, the SpO2 decreases and the need for oxygen in the inspiratory air (FiO2) increases. Other indicators help to further assess the patient's hypoxia, such as: PaO2, PaO2/FiO2 ratio, oxygen index (OI=FiO2 x MAP x 100/PaO2).... Can also be used indicators such as SpO2/FiO2 ratio or oxygen saturation index (OSI = FiO2 x MAP x 100/SpO2) in case blood gas cannot be made.
Many studies have demonstrated the correlation between SpO2/FiO2 and PaO2/FiO2 as well as between OI and OSI. Another feature of patients with ARDS at this stage is the phenomenon of “hard lung”. Decreased lung elasticity can be detected by observing thoracic mobility, monitoring the need for inspiratory pressure to achieve a desired tidal volume (Vt), or monitoring the complience index on a machine. breath for assessment.

During this stage, in addition to severe respiratory failure, patients with ARDS often have symptoms of multi-organ dysfunction such as circulatory failure, myocardial dysfunction, renal failure, and disorder. electrolytes , blood clotting disorders ...
Inflammatory processes in the pathogenesis of ARDS in addition to damage to alveolar cells and capillary endothelial cells can also damage other organs, including the liver , kidney, brain, blood and immune system. However, other organ failure is mainly a consequence of respiratory failure causing tissue hypoxia. The brain and heart are two organs that are sensitive to hypoxia, so they usually manifest first. Other organs such as liver, kidney... can also be the result of hypoxia, although it may manifest later. Patients with ARDS may die during this stage from severe hypoxia or from multi-organ failure.
2.3 Fibrosis and Recovery Stage Patients who survive the full-blown stage will progress to the fibrosis and convalescence phase. The earliest manifestation of this convalescent phase is an improvement in breathing and blood oxygen measurements.
The mechanical ventilation indicators gradually decreased and the patient was weaned off the machine. However, at this stage, the patient may develop alveolar fibrosis and progressive interstitial space. Occasionally forms cysts and emphysema. The time it takes for a patient to fully recover depends on the degree of fibrosis in the lung and the complications caused by the fibrosis.
As soon as the initial symptoms of the disease appear, you should immediately go to a reputable medical facility for examination and treatment. Vinmec International General Hospital is a high-quality medical facility in Vietnam with a team of highly qualified medical professionals, well-trained, domestic and foreign, and experienced.
A system of modern and advanced medical equipment, possessing many of the best machines in the world, helping to detect many difficult and dangerous diseases in a short time, supporting the diagnosis and treatment of doctors the most effective. The hospital space is designed according to 5-star hotel standards, giving patients comfort, friendliness and peace of mind.
Để đặt lịch khám tại viện, Quý khách vui lòng bấm số HOTLINE hoặc đặt lịch trực tiếp TẠI ĐÂY. Tải và đặt lịch khám tự động trên ứng dụng MyVinmec để quản lý, theo dõi lịch và đặt hẹn mọi lúc mọi nơi ngay trên ứng dụng.
Dịch vụ từ Vinmec
-
 Hội chứng suy hô hấp cấp tiến triển (ARDS)
Hội chứng suy hô hấp cấp tiến triển (ARDS)Những năm gần đây, hồi sức nội khoa xuất hiện hội chứng bệnh lý ở phổi rất đặc biệt, có tên là hội chứng suy hô hấp cấp tiến triển ARDS. Hội chứng được mô tả năm 1967 này đến ...
Đọc thêm -
 Lý do dễ bị viêm phổi do vi khuẩn sau nhiễm virus
Lý do dễ bị viêm phổi do vi khuẩn sau nhiễm virusKhi bị sốt nhẹ, cảm cúm, nhiều người chủ quan xem nhẹ bệnh hoặc uống qua loa và viên thuốc. Tuy nhiên, với những triệu chứng đó, chúng ta không nên xem thường, bởi có thể sau khi nhiễm virus ...
Đọc thêm -
 Viêm phổi do vi khuẩn ở trẻ em
Viêm phổi do vi khuẩn ở trẻ emViêm phổi là một bệnh nhiễm khuẩn ở phế quản và nhu mô phổi, tổn thương thường lan tỏa, rải rác hai phổi làm rối loạn trao đổi khí gây suy hô hấp. Viêm phổi trẻ em có thể chữa ...
Đọc thêm -
 Làm sao phân biệt được viêm phổi do vi khuẩn? Cần những xét nghiệm nào?
Làm sao phân biệt được viêm phổi do vi khuẩn? Cần những xét nghiệm nào?Chào bác sĩ! Tôi muốn hỏi làm sao phân biệt được viêm phổi do vi khuẩn? Cần những xét nghiệm nào? Vì sau khi chụp X quang 2 tư thế đứng và thổi khí, bác sĩ thấy tôi bị viêm ...
Đọc thêm -
 Viêm phổi ở trẻ mới biết đi
Viêm phổi ở trẻ mới biết điTừ viêm phổi có nghĩa là "nhiễm trùng phổi." Do nhiễm trùng, các đường dẫn khí nhỏ trong phổi bị sưng lên và tạo ra nhiều chất nhầy. Chất nhầy chặn đường thở và làm giảm lượng oxy có thể ...
Đọc thêm