
Purulent pleurisy: Diagnosis and treatment
The article is professionally consulted by Master, Doctor Nguyen Huy Nhat - Department of Medical Examination & Internal Medicine - Vinmec Danang International General Hospital.
1. What is empyema?
The cause of empyema may be an infection of the pleura or a complicated infection in the lung parenchyma that has spread to the pleural space. Regardless of the cause, it is generally a serious infection that can lead to sepsis with a high mortality rate of 15% to 20%.

2. How to diagnose empyema?
Some cases of empyema have a more prolonged history, mainly of weight loss, decreased appetite, and vague discomfort. These symptoms are sometimes nonspecific and may be similar to a multitude of other conditions, including pleural tuberculosis or pleural malignancy. At this time, the median time between symptom onset and patient arrival at the hospital was more than two weeks.

3. What laboratory tests help diagnose empyema?
Concurrently, all patients should receive a peripheral blood culture. A positive blood culture is the hallmark of sepsis, occurring in approximately 15% of patients with empyema.
3.2. Examination of pleural fluid Fluid or pus in the pleural cavity is removed to perform tests to determine the nature of the fluid as exudative or permeable and the cause of its formation. Sometimes the pleural puncture also helps to decompress and increase the gas exchange volume for the side of the lung that is compressed by the effusion, helping the patient to improve symptoms significantly.
If an infection is suspected, the fluid will be cultured with bacteria, doing a TB PCR test to look for integrated pathogens. Likewise, cytological staining and microscopic analysis can help indicate effusions of malignancy.

Thoracic ultrasound: Pleural ultrasound can detect low pleural fluid volumes with higher sensitivity than chest X-ray. Not only that, pleural ultrasound also facilitates the accurate localization of pleural fluid, orients the pleural puncture needle for testing with many advantages, reducing the risk of organ perforation and pneumothorax. pleura.
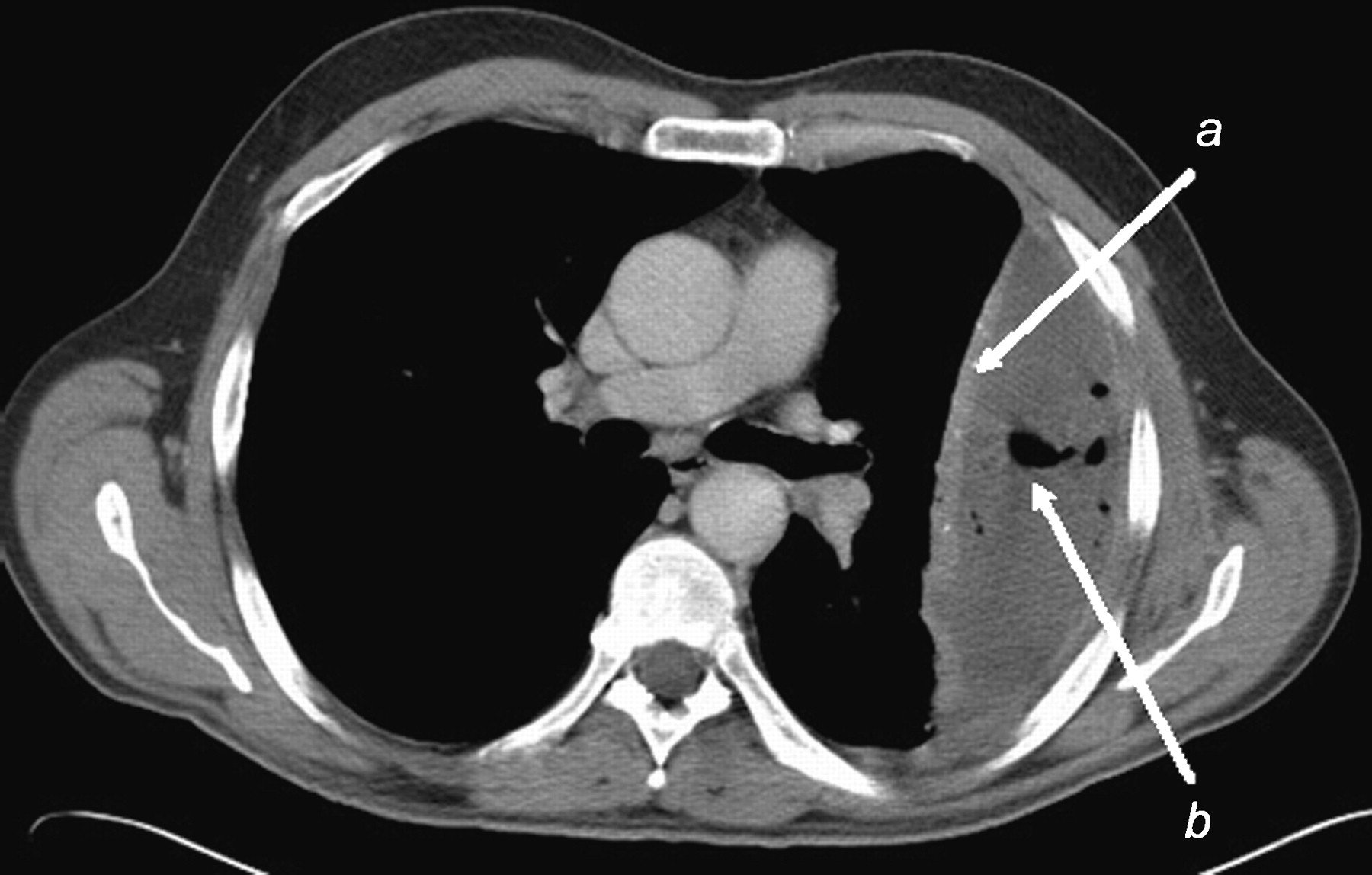
Computed tomography: An air-window thoracic CT is extremely helpful in patients with ambiguous chest X-ray or ultrasound images. CT usually shows lenticular fluid with compression of surrounding lung parenchyma and pleural thickening occurring in 56-100% of cases. In addition, CT is useful in differentiating between peripheral lung abscess and pleural infection. The detached pleural sign found in empyema is helpful in identifying discontinuity with the lung abscess.
4. Differential diagnosis of empyema with what diseases?
Malignancy: One of the most common analogues of pleural infection is pleural disease. malignant . Patients with pleural malignancies often present with fever and signs of inflammation and pleural effusion. Biochemical analysis of such effusions may be indistinguishable from pleural infection, especially in active malignancy with poor prognosis.
Isolated pleurisy: Patients with inflammatory conditions in other organs, such as rheumatoid arthritis, may present with pleural effusion and elevated inflammatory markers in the blood along with shortness of breath. , cough, chest pain. Low pH and glucose in the pleural fluid are characteristic although patients also often have other signs of rheumatoid arthritis at flare-ups.

5. Guidelines for the treatment of empyema
Long-term broad-spectrum antibiotic therapy Diagnostic pleural effusion and decompression Surgical intervention Early surgery when indicated Nutritional support Prophylaxis against venous thrombosis Details of each treatment goal are presented below:
The empiric chosen antibiotic should be determined by considering whether the infection is community- or healthcare-associated, the prevalence of local bacterial infections, and their resistance patterns . In particular, community-acquired pathogens are often sensitive to beta-lactams in combination with beta-lactamase inhibitors, such as amoxicillin and clavulanic acid or piperacillin-tazobactam. Metronidazole is usually indicated if coinfection with anaerobic organisms is suspected. In cases where empyema is medically relevant, resistant strains of bacteria, including gram-negative enterococci and MRSA, cannot be ruled out. At this point, a reasonable antibiotic option is carbapenem in combination with vancomycin.

In the past, larger tubes were often used to drain empyema, but recent evidence supports small tubes (less than 15 F) to be equally effective with less pain. .
Drainage procedures should be conducted under the guidance of imaging, usually ultrasound, to help the collection area easily be located, limiting the risk of perforation of nearby organs as well as air emphysema. pleural pressure.
5.3. Surgical intervention Up to 30% of patients with empyema require early surgery when the infection is difficult to control with conventional drainage and the risk of sepsis is very high.
Although there is currently no evidence that timing or clinical endpoints play a role as an indication for surgical intervention in cases of empyema, the patient's condition is unlikely to improve clinically and X- Phototherapy after seven days of treatment is usually applied. In contrast, patients with only very little residual pleural fluid but improved clinical and laboratory parameters, the amount of pus will be resolved gradually over time under the effect of antibiotics and the immune system of patients. body.

Although specific nutritional therapy in the setting of empyema has not been formally tested, nutritional support, including nasogastric tube feeding in these cases, should be considered. , both increase the energy needed to absorb during the day, fight against catabolism, and prevent the risk of pneumonia associated with aspiration.
In summary, empyema is a relatively severe inflammatory condition that requires early multimodal diagnosis and aggressive antibiotic treatment from the outset. If the patient has significant empyema, drainage as well as surgical intervention should be performed early. Only then can empyema be controlled, minimizing the risk of sepsis as well as preserving the patient's life.
Doctor Nguyen Huy Nhat has many years of experience in the field of respiratory disease treatment at Hue Central Hospital, Hoan My General Hospital, .. before being a doctor of General Internal Medicine Department of General Hospital. Vinmec Da Nang International
For detailed advice on empyema, please come directly to Vinmec health system or book online HERE.
Reference source: medicalnewstoday.com
SEE MORE:
Find out information about empyema Signs and causes of pleurisy How is pleurisy diagnosed and treated?
Dịch vụ từ Vinmec
-
 Công dụng thuốc Medbactin
Công dụng thuốc MedbactinMedbactin thuộc nhóm thuốc chống nhiễm khuẩn, trị ký sinh trùng, kháng virus và kháng nấm. Thuốc có dạng bào chế viên nén bao phim, đóng gói hộp 1 vỉ x 4 viên. Trước khi sử dụng thuốc Medbactin, người ...
Đọc thêm -
 Công dụng thuốc Klavunamox Pediatric
Công dụng thuốc Klavunamox PediatricThuốc Klavunamox Pediatric là bột pha hỗn dịch uống chứa thành phần Amoxicillin và Acid clavulanic, được chỉ định để điều trị nhiễm trùng ở trẻ em. Tìm hiểu một số thông tin về công dụng, liều dùng và lưu ...
Đọc thêm -
 Công dụng thuốc Cefadromark
Công dụng thuốc CefadromarkThuốc Cefadromark có thành phần chính là kháng sinh cephalosporin thế hệ 1. Thuốc có phổ tác dụng trung bình trên các vi khuẩn gram dương và số ít các vi khuẩn gram âm. Kháng sinh Cefadromark được chỉ định ...
Đọc thêm -
 Công dụng thuốc Clintaxin
Công dụng thuốc ClintaxinHiện nay có nhiều loại kháng sinh trên thị trường thuốc, trong đó có Clintaxin. Cùng tìm hiểu rõ hơn công dụng thuốc Clintaxin, Clintaxin trị bệnh gì, thuốc Clintaxin dùng thế nào... ngay sau đây.
Đọc thêm -
 Công dụng thuốc Cefalvidi
Công dụng thuốc CefalvidiThuốc Cefalvidi thuộc nhóm kháng sinh, kháng virus, kháng nấm chứa thành phần chính là Cefadroxil. Cefalvidi thường được dùng để điều trị các tình trạng nhiễm khuẩn tiết niệu, hô hấp, da và mô mềm hoặc viêm xương tuỷ, ...
Đọc thêm