
Cytomegalovirus pneumonia - Part 1
Congenital CMV infection from mother, organ transplant children The highest rate of CMV pneumonia as well as the highest severity occurs in lung transplant patients. It can be classified into primary pneumonia and recurrent pneumonia. On rare occasions, CMV can cause community-acquired pneumonia in individuals with influenza and adenovirus, and in severe cases of viral pneumonia.
CMV pneumonia is defined as symptoms of lung disease when laboratory tests detect CMV antigens in bronchial fluid or lung parenchyma. Detection of CMV should be through culture, histopathology, immunohistochemical analysis or in situ hybridization techniques.
I. Clinical symptoms
Most cases of viral pneumonia are initiated by symptoms of upper respiratory tract infection within a few days (rhinitis and cough). This stage usually lasts for 2-3 days with symptoms: cough, low-grade fever and runny nose, then pneumonia.
In transplant patients, illness usually begins 1-3 months after transplantation and begins with fever and dry cough. The disease progresses rapidly with chest indrawing, dyspnea, and hypoxia becoming prominent.
The disease usually lasts more than 1 week, antibiotic treatment and conventional drugs do not improve.
In the full-blown phase, the clinical symptoms are often atypical, the following may be present:
Systemic symptoms: + Fatigue.
+ Eat poorly.
+ Sweat a lot.
+ Muscle and joint pain.
Functional symptoms: + Fever is usually not as high as bacteria, some patients have no fever.
+ Ho.
+ Some cases have skin rash.
+ May have green skin.
+ Liver and spleen enlargement are common symptoms in more than 80% of patients, liver enlargement is about 3.5cm, no signs of liver prolapse.
+ Diarrhea.
+ Wheezing.

Physical symptoms: + There may be symptoms of respiratory failure, cyanosis, dyspnea, dyspnea on exertion.
+ Chest retraction.
+ Lack of oxygen due to decreased oxygen levels in the blood. This sign is often severe and indicates a risk of death (especially in mechanically ventilated patients).
+ Auscultation of the lungs may have small-grained moist rales, sometimes with hissing rales.
+ CMV pneumonia is often co-infected with other bacteria, such as P.carinii.
+ Pneumonia is common in immunocompromised patients such as chemotherapy patients 22,23,60.
In general, it is clinically difficult to distinguish between viral pneumonia and pneumonia.
II. Subclinical
Diagnostic test to confirm CMV pneumonia: + CMV antigen in body fluids.
+ Microbiological tests: PCR-CMV of oropharyngeal lavage fluid, bronchial fluid; CMV ELISA; endotracheal inoculation.
+ Pathology.
Tests to monitor treatment: + Arterial blood gases.
+ CTM.
+ Blood biochemistry: Serum Bilirubin, AST, ALT, Urea, Creatinine
+ Humoral immunity (IgM, IgA, IgG), 9CD4, CD8 cell immunity
+ Imaging: X-ray, CT lung scan
1. Arterial blood gas
Possibly a decrease in SpO2, in the case of respiratory failure due to decreased gas exchange in the alveoli of the lungs, there will be many changes in blood gas indices.

2. Hematology test
Blood chemistry + LDH is elevated in more than 90% of cases, averaging 450 IU/L.
+ Liver function, liver enzymes may increase.
+ Kidney function.
+ Blood protein may decrease due to poor feeding.
Erythrocyte sedimentation rate and CRP are normal or slightly increased. Complete blood count and white blood cell count show normal or slightly increased white blood cell count (< 20,000/mm3) with lymphocyte predominance.
3. Diagnostic Imaging
3.1 Cardiopulmonary X-ray The diagnosis of CMV pneumonia should suggest a chest radiograph, but this diagnostic method cannot distinguish them from other causes of pneumonia in immunocompromised patients.
A chest x-ray with pneumonia along with a positive CMV test can help confirm the diagnosis.
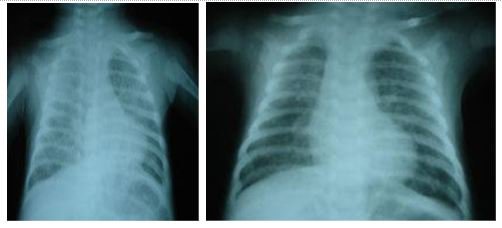
Clinical symptoms are seen in most cases. Usually presents with bilateral lung involvement.
Predominantly interstitial lung lesions, often with bilateral diffuse infiltrates. Alveolar solidification accounts for 25%. The image of blurred glass can be seen in some cases Nodular lesions in 10% of cases Pleural effusion is also quite common. Hilar lymph node involvement may be present. 3.2 CT SCAN is a more sensitive diagnostic method for pulmonary infiltrates. Valuable in patients with hypoxia and no infiltrates on plain chest radiographs. With high resolution CT can find lesions that are not normally seen on radiographs.
4. Virus isolation
Specimen: throat wash, bronchoalveolar lavage, urine. Inoculation of the specimen into the cells and observing the cell changes after 1-2 weeks will give the image of swollen cells containing many inclusions in the nucleus. Because cell destruction occurs slowly (1-2 weeks), the disadvantage of this method is the long time to read results. Virus isolation combined with seroconversion is the best method for the primary diagnosis of CMV infection in normal people.
5. Shell vial assay
Although culture is highly sensitive, clinical isolates of CMV can be slow growing, requiring 6 weeks of incubation in a virology laboratory. The culture adaptation provides faster results than the monoclonal antibody-enhanced centrifugation technique, known as shell vial assay. In this technique, patient samples are centrifuged on top of a single layer of cells (in practice, the patient samples are concentrated). Then, after incubation in the culture, cells are stained with a monoclonal antibody specific to a cytomegalovirus antigen, usually an immediate gene product. A positive shell vial culture is evidence of active cytomegalovirus infection, and this test is a useful addition to traditional viral culture methods.

Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, a system of modern equipment and technology. The hospital provides comprehensive and professional medical examination, consultation and treatment services, with a civilized, polite, safe and sterile medical examination and treatment space. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.
Để đặt lịch khám tại viện, Quý khách vui lòng bấm số HOTLINE hoặc đặt lịch trực tiếp TẠI ĐÂY. Tải và đặt lịch khám tự động trên ứng dụng MyVinmec để quản lý, theo dõi lịch và đặt hẹn mọi lúc mọi nơi ngay trên ứng dụng.
Dịch vụ từ Vinmec
-
 Chẩn đoán CMV ở mẹ và thai nhi
Chẩn đoán CMV ở mẹ và thai nhiQuá trình lây nhiễm virus CMV (Cytomegalo) có thể diễn ra trong suốt quá trình mang thai. Do đó, nếu mẹ bị nhiễm CMV càng sớm thì trẻ sẽ có nguy cơ gặp các vấn đề về sức khỏe cũng ...
Đọc thêm -
 Chỉ số men gan của trẻ là 75 có sao không?
Chỉ số men gan của trẻ là 75 có sao không?Con nhà em mới hơn 2 tháng tuổi. Hiện nay, bé có triệu chứng virus CMV gây nên men gan cao, hiện tại chỉ số men gan là 75. Vậy bác sĩ cho em hỏi chỉ số men gan của ...
Đọc thêm -
 Có tái nhiễm virus CMV trong lần mang thai tiếp không? Đã tiêm vacxin Viêm gan B có cần tiêm lại không?
Có tái nhiễm virus CMV trong lần mang thai tiếp không? Đã tiêm vacxin Viêm gan B có cần tiêm lại không?Em vừa đình chỉ thai kỳ ở tuần 29 được 1 tháng do nhiễm virus CMV. Em đã tiêm 3 mũi vacxin viêm gan B vào năm 2014 và từ đó chưa tiêm thêm. Vậy bác sĩ cho em hỏi ...
Đọc thêm -
 Thuốc Prevymis: Công dụng, chỉ định và lưu ý khi dùng
Thuốc Prevymis: Công dụng, chỉ định và lưu ý khi dùngThuốc Prevymis là thuốc điều trị virus CMV, tránh được nguy cơ mắc các bệnh do loại virus này gây ra. Việc sử dụng thuốc điều trị virus CMV cần tuân thủ nghiêm ngặt chỉ định của bác sĩ để ...
Đọc thêm -
 Trẻ nhiễm virus CMV có nguy hiểm không?
Trẻ nhiễm virus CMV có nguy hiểm không?Bé nhà em được 1 tháng 20 ngày. Hiện tại, bé đang bị viêm phổi và có làm xét nghiệm máu bị nhiễm virus CMV IgM 7,68 (s/co), IgG 123,96 (Au/ml). Vậy bác sĩ cho em hỏi trẻ nhiễm virus ...
Đọc thêm