The article was written by MSc. Dr. Mai Vien Phuong - Gastroenterologist, Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
The introduction of flexible endoscopes has made it possible to observe the interior of the stomach and colon, allowing for accurate diagnoses of both benign and malignant diseases. Advancements in pathological anatomy enable us to examine specimens under a microscope, helping to determine the histological nature of tissue samples or lesions and to distinguish between benign and malignant conditions. The assessment of potential malignancy is based on various factors, including the mobility, surface characteristics, and shape of the polyp, as well as the results obtained from staining and magnification techniques.
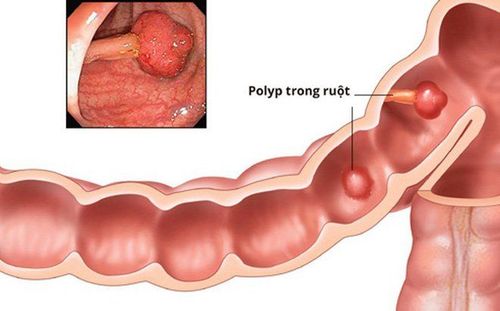
1. What is a colon polyp?
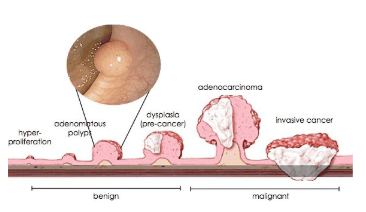
A colon polyp is a small mass of cells that forms on the lining of the colon (large intestine). Most colon polyps are harmless, but over time, some colon polyps can develop into colon cancer, which is fatal when found in its late stages. There can be one or more colon polyps. Anyone can get colon polyps.
Colon polyps often do not cause symptoms. It is important to have regular screening, such as colonoscopy, because colon polyps found early can often be completely and safely removed. Regular screening for colon cancer is a good way to prevent colon cancer.
2. Why do we need to carefully evaluate polyps before removing polyps?
The colon wall consists of the mucosa, submucosa, muscle layer, and serosa. According to research, removing lesions that have not invaded the mucosal layer will have a very good prognosis.
For endoscopists, when polyps are discovered, it is essential to evaluate them carefully before proceeding with removal. This precaution is necessary to avoid cutting polyps that may be beyond the appropriate indication for resection.
Some polyps are very small, around 5 mm in size. Typically, these smaller polyps are less likely to become malignant; however, they may still have surface cancer that is only detected through pathological results following complete removal. In such cases, the patient may need further tests, such as abdominal and pelvic CT scans, as well as blood tests for CEA and CA 19-9, to assess the stage of the lesion. If the polyp is found to be invasive, surgery may be required to remove the segment of the intestine containing the cancerous lesion.
If lesions are correctly assessed from the outset, patients may avoid unnecessary polypectomy, which incurs costs, requires time, and presents risks associated with the procedure.
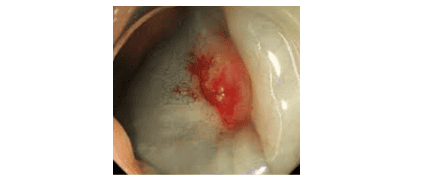
3. Characteristics of Cancerous Polyps on Conventional Endoscopic Images
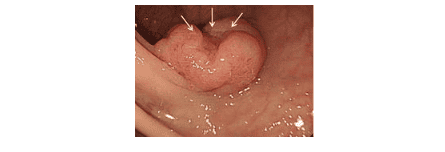
Certain characteristics may indicate cancerous polyps: the surface may be spreading, exhibit ulcers or erosions, or show converging intestinal mucosal folds. Additionally, “solid” polyps and concave polyps with a raised center are concerning.
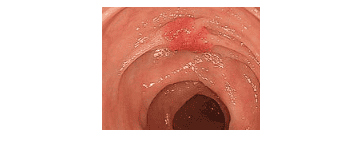
Source: Saito, S. et al. "Endoscopic features of submucosal deeply invasive colorectal cancer with NBI characteristics." *Clinical Journal of Gastroenterology*, volume 8, pages 353–359 (2015).
Endoscopists should exercise caution before cutting such polyps, as invasive cancer may have reached the submucosal layer, and endoscopic removal may not ensure safety from cancerous surfaces.
4. Evaluation of Polyps by Magnifying Endoscopy and Color Endoscopy
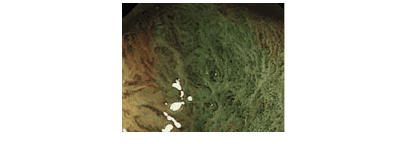
With advancements in endoscopy technology, including electronic lesion staining modes (NBI function) and magnification capabilities up to 100 times, we can achieve more detailed assessments of lesions.
Japanese researchers have classified polyps based on surface and blood vessel characteristics, using various systems such as Sano classification, Hiroshima classification, Kudo classification, JNET classification, and the NICE classification globally to evaluate the malignancy of polyps.
Polyps displaying irregular microsurfaces which are indicated by dilated, twisted, or broken surface blood vessels, or uneven diameters, are classified as having a risk of submucosal invasion. Endoscopic resection of these polyps may not ensure safe outcomes.
5. Evaluation of Polyps by Endoscopic Ultrasound
The introduction of endoscopic ultrasound has opened up new opportunities for advancements in endoscopy. In this technique, an ultrasound probe is integrated into the tip of the endoscope, transmitting data to a server for analysis.
Cancerous polyps often invade the deeper layers of tissue. The ultrasound probe is positioned near the lesion, allowing for assessment of the invasion level into the submucosa and muscle layer of the digestive tract wall. This information helps determine whether the polyp can be removed endoscopically.
6. Evaluation of Polyps by the “Lifting Injection” Method – “Non-Lifting Sign”
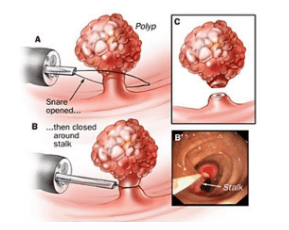
In the endoscopic mucosal resection (EMR) technique, used to excise sessile polyps, a specific solution is injected into the submucosa. This injection is intended to lift the lesion within the mucosal layer, preventing complications such as perforation of the digestive tract during the procedure.
If the solution is injected but the lesion does not lift, the polyp has likely invaded or fibrosed into the submucosa. In these cases, caution is warranted, as the polyp may be cancerous.
The techniques described above are utilized at Vinmec Hospital System to assess the malignancy of polyps before removal. For polyps suspected of being malignant, rather than excising the polyp, the endoscopist will biopsy the suspicious area on the surface to guide further treatment.
7. Treatment of Colorectal Polyps at Vinmec Central Park
At Vinmec Central Park Hospital, a highly trained team of doctors specializes in the diagnosis and treatment of early gastrointestinal cancer and colorectal polyps. The hospital is equipped with state-of-the-art digestive endoscopy systems from Olympus, a leading brand in the field, including the Olympus CLV 190 endoscopy system.
One advantage of these endoscopy machines is their narrow band of light (NBI), which provides high-resolution and high-contrast images. This enhances the ability to detect, screen, and diagnose digestive cancers at early stages. When a cancerous lesion is detected early, depending on the characteristics of the polyp, it can be removed using mucosal resection (EMR) or submucosal dissection (ESD) via a flexible endoscope, avoiding the need for surgery.
Furthermore, to ensure the sterility of the endoscopes, the hospital is equipped with an automatic endoscope cleaning machine and a reverse osmosis (RO) water filtration system.
Patients are welcome to visit Vinmec Central Park for an examination or can contact the hotline at 0283 6221 166 for assistance.
If you need consultation and examination at other Vinmec Hospitals in the healthcare system nationwide, please make an appointment on the website to be served.
To arrange an appointment, please call HOTLINE or make your reservation directly HERE. You may also download the MyVinmec app to schedule appointments faster and manage your reservations more conveniently.
To arrange an appointment, please call HOTLINE or make your reservation directly HERE. You may also download the MyVinmec app to schedule appointments faster and manage your reservations more conveniently.