Duodenal gallbladder fistula is an abnormal spontaneous communication between the biliary system and the gastrointestinal tract. In some cases, gallbladder fistula can be a rare complication of untreated gallstones. These fistulas lead to diverse clinical manifestations and can pose a life-threatening risk to patients.
1. What is a Duodenal Gallbladder Fistula?
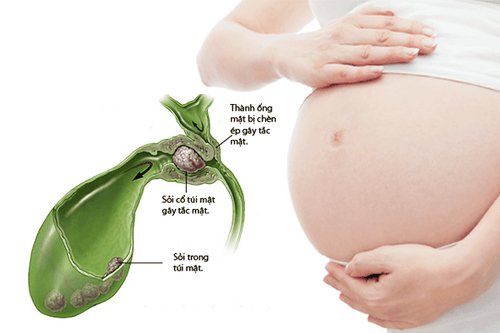
A gallbladder fistula consists of chronic ulcer-like tracts between the gallbladder and adjacent organs. These fistulas can connect the gallbladder with the biliary system, but rarely involve the digestive tract (internal fistula) or the abdominal wall (external fistula). A duodenal gallbladder fistula occurs when there is an abnormal connection between the gallbladder and the duodenum, where bile from the common bile duct enters the digestive tract.
In most cases, gallbladder fistula is a rare complication of biliary stones or neoplastic lesions and is classified as primary or secondary. Internal fistulas, such as duodenal gallbladder fistulas, are typically caused by inflammation and often arise as late complications of gallstones or tapeworm infections. Additionally, surgical interventions on the bile ducts, such as laparoscopic cholecystectomy, can lead to secondary gallbladder fistulas.
2. How is Duodenal Gallbladder Fistula Diagnosed?
Preoperative diagnosis of gallbladder or biliary fistulas, including duodenal gallbladder fistulas, remains challenging, with a detection rate of only 8–17% of cases. Patients often present with symptoms of gallstones, including persistent right upper quadrant abdominal pain, colicky pain that worsens after meals, nausea, bloating, and indigestion. Mirizzi syndrome may also be observed in some cases.
A key diagnostic clue is a history of previous biliary surgical intervention. To establish an accurate diagnosis and effective treatment plan, physicians need to determine the following:
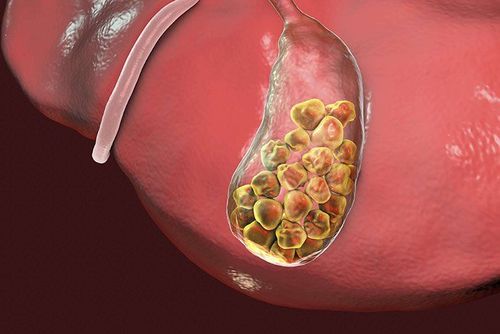
- Cause of the gallbladder fistula: The presence of gallstones is the most common underlying condition. If gallstones are absent, other causes such as infections or malignancies should be investigated.
- Degree of biliary obstruction and the extent of gallbladder wall erosion or destruction.
- Presence of a bidirectional fistula opening.
The following diagnostic tests are commonly used to evaluate these factors: - Abdominal ultrasound: A non-invasive diagnostic tool to detect the presence of gallstones.
- Magnetic resonance cholangiopancreatography (MRCP): A more accurate imaging modality (approximately 50% sensitivity) that provides detailed anatomical information about the biliary system and gallbladder. MRCP can also help identify the degree of obstruction and rule out neoplastic lesions at the liver hilum or within the liver parenchyma that may invade the gallbladder.
- Invasive procedures: Endoscopic ultrasound and endoscopic retrograde cholangiopancreatography (ERCP) offer higher diagnostic accuracy for detecting gallbladder fistulas, including duodenal gallbladder fistulas. ERCP is particularly useful for diagnosing primary biliary fistulas and plays both a therapeutic and surgical role by allowing stone removal after sphincterotomy and bile duct stent placement.

3. How is Duodenal Gallbladder Fistula Treated?
Surgical intervention is the only definitive treatment for duodenal gallbladder fistula. However, managing primary biliary fistulas remains a significant challenge for most surgeons.
A thorough understanding of the pathology, biliary tract anatomy, and its relation to other digestive organs is essential. Inflammatory changes in Calot's triangle often result in substantial anatomical distortion, making surgical control of lesions difficult.
The fundamental principle of surgery for duodenal gallbladder fistula is biliary drainage reconstruction, typically involving:
Cholecystectomy (gallbladder removal), restoration of the duodenum, stone removal, decompression of any compressive masses, and elimination of inflammatory sources. Depending on the clinical presentation, surgeon expertise, and available facilities, patients may undergo retrograde cholecystectomy, laparoscopic surgery, or open abdominal surgery.
Postoperatively, patients may require placement of a biliary drainage tube to ensure proper structural and functional recovery of the biliary system. If uncontrolled intra-abdominal infections are present, a peritoneal drain may also be placed, though these tubes are typically removed before hospital discharge.
Following surgery, patients require regular follow-ups, imaging assessments, and laboratory tests to ensure successful recovery and to detect potential complications.
In conclusion, duodenal gallbladder fistula is an uncommon condition characterized by an abnormal communication between the gallbladder and the duodenum. It typically results from chronic gallbladder inflammation, most commonly due to gallstones. Diagnosis primarily relies on ultrasound imaging, confirmed by computed tomography (CT). The main treatment approach is surgical intervention, with postoperative monitoring essential to prevent recurrence.
To arrange an appointment, please call HOTLINE or make your reservation directly HERE. You may also download the MyVinmec app to schedule appointments faster and manage your reservations more conveniently.