This article has been professionally consulted by Dr. Le Thanh Cam - Grade II Specialist- Pediatric Department - Vinmec International General Hospital Da Nang.
Post-tonsillectomy hemorrhage is not an uncommon issue and may be prolonged. In most cases, the bleeding is minimal, and it may only be detected by observing a small amount of blood on the tongue. However, if significant bleeding occurs, accompanied by coughing, vomiting blood, or persistent hemorrhage, it is imperative to seek immediate medical attention.
1. Indications for Tonsillectomy
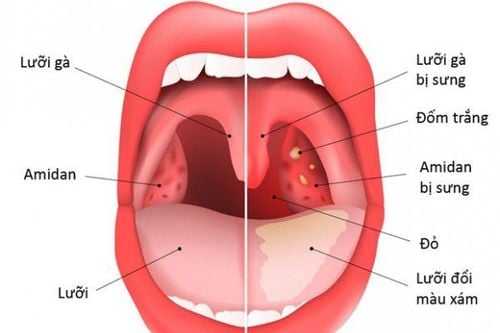
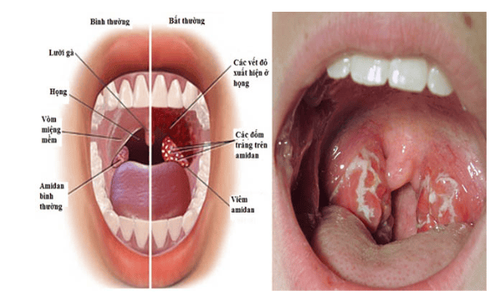
The tonsils serve as an immunological barrier in the oropharyngeal region. When the tonsils respond to the infiltration of pathogens into the nasal and pharyngeal areas excessively, tonsillitis occurs, characterized by swelling and erythema. The destruction of bacteria within the tonsils often results in necrotic tissue manifesting as foul-smelling pus. Repeated episodes of tonsillitis can weaken the tonsils' antibacterial defense, and the inflammatory foci present within the tonsils can serve as a source for recurrent pharyngeal infections.
The etiology of tonsillitis may include upper respiratory infections, viral infections, and influenza. Patients with tonsillitis may present with symptoms such as:
- High fever exceeding 39-40°C
- Swollen and erythematous tonsils, possibly with white pseudomembranes
- Dry throat, sore throat, dysphagia, and headaches localized to the temples
- Nasal obstruction, nasal discharge initially clear, which later becomes thicker, white, or yellow...

As upper respiratory infections can lead to tonsillitis, recurrent tonsillitis, if not treated promptly, may result in complications such as scarlet fever, peritonsillar abscess, acute arthritis, glomerulonephritis, etc. However, not all cases of tonsillitis necessitate a tonsillectomy; this procedure is indicated in specific situations:
- Frequent episodes, recurrent 5-6 times per year
- Development of peritonsillar abscess or complications such as otitis media, sinusitis, or severe complications such as rheumatic fever, arthritis, glomerulonephritis
- Enlarged tonsils obstructing the airway, causing snoring, sleep apnea, or recurrent infections significantly impacting the patient's quality of life...
- Tonsils with numerous crypts harboring secretions causing halitosis, dysphagia, or suspected malignancy...
2. Causes of Hemorrhage Post-Tonsillectomy
Possible incorrect indications may involve:
- The causes of hemorrhage following tonsillectomy may include active throat inflammation.
- Patients with hematological disorders or individuals currently menstruating.
Technical errors may include:
- Residual tonsil tissue post-resection
- Disruption of the anterior and posterior pillars (musculature of the soft palate); unstitched tears may lead to persistent, albeit minimal, bleeding
- Penetration of the lateral pharyngeal wall, including the fascia and constrictor muscles, causing damage to internal vessels resulting in post-tonsillectomy hemorrhage.
- Utilization of a clamp technique may improperly navigate, failing to adhere to designated dissection planes, potentially damaging critical structures posterior to the tonsils, such as the internal carotid artery
- Injury to the ascending palatine artery and the tonsillar branches could result in post-tonsillectomy bleeding, sometimes requiring external carotid artery ligation
- Excessive tearing of the anterior pillar adjacent to the midline during dissection may jeopardize the descending palatine artery.
3. Management and Monitoring of Post-Tonsillectomy Hemorrhage

3.1. Monitoring Post-Tonsillectomy
- Close monitoring for early hemorrhage should occur within the first 24 hours post-tonsillectomy.
- Post-operatively, patients should avoid strenuous activities and should lie laterally without head elevation to prevent trauma to the surgical site leading to bleeding.
- In the initial two days, patients should consume milk; the subsequent three days may consist of thin porridge, and from the seventh day onward, patients may gradually transition to a soft rice diet. Normal dietary intake can usually resume after ten days, while avoiding acidic, spicy, salty, hot, and hard foods.
- Typically, post-tonsillectomy hemorrhage may manifest 7 days later or potentially sooner or later; at this point, prompt evaluation and intervention are required.
3.2 Management of Post-Tonsillectomy Hemorrhage
Local Management:
- In the event of hemorrhage following tonsillectomy, patients should be instructed to suck on small ice cubes, swallowing or spitting them out, or alternatively, applying ice cubes in a plastic bag to the neck area for compression.
- Utilize gauze soaked in a hemostatic solution such as hydrogen peroxide, applying firm pressure to the tonsillar fossa at the site of bleeding for approximately 10 minutes.
- Administer 1 ml of 1% novocaine combined with adrenaline directly at the hemorrhaging site to constrict the capillaries and facilitate hemostasis.
- Employ Kocher clamps without ratchet, measuring 17 cm, to grasp the precise area of hemorrhage for one hour. Should bleeding persist after removal, suture ligation is necessitated.
- Ligation of blood vessels is specifically indicated for arterial or venous bleeding, occurring at the superior pole or pedicle of the tonsil during or following surgical intervention. The sutures will naturally dissolve after 7 days.
- Apply Boisviel compression clamps for bleeding at the tonsillar pedicle and in the deep recesses of the palatine tonsil.

- Utilize electrocautery by applying Kocher clamps at the site of bleeding. The inactive electrode is placed on one hand of the patient, while the active electrode of the electrocautery device is directed towards the Kocher clamp, resulting in the tissue at the clamp's tip being cauterized and the blood vessel being coagulated.
- Perform the Tarneaud method for approximating the two pillars, executing two or three mattress sutures (either catgut or non-absorbable suture) passing from the posterior pillar to the anterior pillar, subsequently tying the pillars together, with a strip of gauze inserted between them. The sutures should be placed approximately 5 mm from the free edge of the pillar. If regular gauze and conventional sutures are used, the gauze is removed after 24 hours, and sutures are excised after 3 days.
- External carotid artery ligation or embolization should only be employed after all aforementioned hemostatic methods have failed.
Systemic Management:
- Administer systemic agents to enhance coagulation.
- Provide cardiac support medications as necessary.
- Infuse saline and glucose intravenous fluids.
- Transfusion of fresh blood should be considered if deemed necessary.
To arrange an appointment, please call HOTLINE or make your reservation directly HERE. You may also download the MyVinmec app to schedule appointments faster and manage your reservations more conveniently.