
Children under 6 years old experience rapid development in physical, mental, and motor domains. Physical growth is typically monitored through biological indicators and growth charts. In addition, psychological tests are used to assess and track psychomotor development. The Denver test is widely used worldwide as a screening tool to identify children at risk of developmental delays.
This article was written by: Resident Doctor Do Van Duc - Psychiatrist, Integrated Mental Health Care Center - Vinmec Times City International General Hospital.
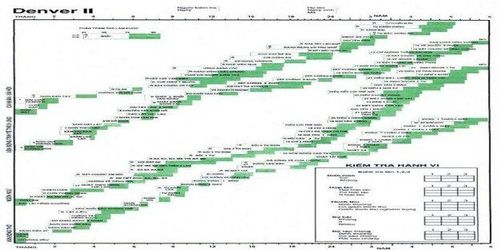
1. What is the Denver Developmental Screening Test?
The Denver Developmental Screening Test was first developed in 1967 at the University of Colorado Medical Center in Denver, USA, and later revised into Denver II in 1992. Due to its simplicity, structured design, and ease of use, it has been widely adopted globally to screen for psychomotor developmental delays in children.
The test is intended to be administered by trained professionals such as child psychiatrists, clinical psychologists, specialized nurses, or developmental intervention specialists.
The Denver Test consists of 125 items divided into four domains:
- Fine motor-adaptive: Hand-eye coordination, manipulation of small objects, control of small muscle groups, and basic problem-solving skills.
- Personal-social: Interaction with others and the ability to meet personal needs.
- Language: Ability to hear, understand, and use language for communication.
- Gross motor: Abilities such as crawling, sitting, walking, running, and coordination of large muscle groups.
The percentage of children able to perform each task at a given age is represented by 25%, 50%, 75%, and 90% markers on the test chart.
2. When is the Denver test used?
The Denver Test is indicated in the following cases:
- Children under 6 years old suspected of having psychomotor developmental delays.
- Children with medical conditions requiring monitoring of developmental progress.
- Children with concerning prenatal or perinatal histories.
Cases where the test should be postponed or not conducted include:
- The child is tired, ill, taking medications affecting mental status, or has severe physical illness.
- The child is unaccompanied by a caregiver or is overly agitated, oppositional, or aggressive.

3. Procedure for Administering the Denver test
The test is conducted by trained professionals such as psychiatrists, psychologists, specialized nurses, or developmental therapists.
Implementation steps are as follows:
3.1. Preparation
The examiner should prepare:
- A suitable testing environment: quiet, well-lit, with appropriate seating or space for the child’s age, and minimal distractions.
- Denver II test form, instruction manual, ruler, pencils, three colored pens (blue, red, purple), and test materials.
3.2. Initial Assessment and Engagement
Before starting:
- Discuss with caregivers: Explain the purpose of the test-that the child does not need to complete all tasks-to reduce pressure on both parents and child.
- Assess the child’s condition: Ensure the child is alert and well enough to participate.
- Build rapport: Approach the child gently and create a relaxed, playful atmosphere so the test feels like a game rather than an exam.
3.3. Test Administration
The examiner selects age-appropriate items from the 125 tasks (not all items are tested). To do this - calculate the child’s exact age (adjust for prematurity if applicable); and draw the age line on the Denver chart.
Testing begins with items to the left of the age line (skills the child is expected to have). If the child fails an item, the examiner moves to easier tasks until the child passes three consecutive items. Then, more difficult items are tested until the child fails three consecutive items.
If the child becomes tired, breaks should be given to ensure accurate results.
Each item is scored as:
- Pass (P): The child successfully performs the task, or the caregiver confirms the child can do it.
- Fail (F): The child cannot perform the task after attempts, or the caregiver confirms inability.
- Refusal (R): The child refuses despite having the ability (due to fear, fatigue, or non-cooperation).
- No opportunity: Used only for caregiver-reported items when the child has not had the chance to try the skill.
The results then can be interpreted as follows by the examiner:
- Advanced: Pass on items entirely to the right of the age line (skills that 90% of peers cannot yet do).
- Normal: Fail or refusal on items to the right of the age line, or where the age line crosses the 25-75% area.
- Caution: Fail or refusal on items in the 75-90% area.
- Delay: Fail or refusal on items entirely to the left of the age line (skills that over 90% of peers can do).
- Evaluate the whole test.
Based on delays and cautions, the examiner will evaluate the whole Denver test according to the following criteria:
- Normal: No delays and at most one caution.
- Suspected delay: One or more delays and/or two or more cautions.
- Untestable: Refusal of more than one item to the left of the age line or in the 75-90% area.
- The test administrator conducts a behavioral assessment: this evaluation is recorded after the test based on the child’s observed behaviors in the rectangular box located at the bottom right corner of the test sheet. To ensure an accurate assessment, the administrator must continuously observe aspects such as the child’s level of cooperation, attention span, interest, and social interaction both before and during the test. The administrator should also ask the parents whether the child’s behavior during the test is consistent with their usual behavior on other days.
The test administrator records the test results in the test form, medical record, or child health booklet, and explains the results to the child’s caregiver.
4. Follow-up after performing the Denver test for psychomotor development assessment
After the evaluation, follow-up is based on the test results as follows:
- Normal: periodic monitoring as advised by a specialist.
- Suspected developmental delay: reassess after 1-2 weeks; if the result still indicates suspected delay, consult a specialist to develop a personalized and specific intervention plan for the child.
- Unable to assess: repeat the test after 1-2 weeks.
Timely screening and intervention are key factors in monitoring and supporting a child’s psychomotor development. At the Integrated Mental Health Care Center, we are always ready to accompany parents and children throughout the screening and assessment process, working together to support each step of the child’s development.
To arrange an appointment, please call HOTLINE or make your reservation directly HERE. You may also download the MyVinmec app to schedule appointments faster and manage your reservations more conveniently.





